Silent Resistance: Rising Antimicrobial Non-Response in Community-Acquired Pediatric UTIs in Europe
Antoine Lefevre¹, Camille Dubois², Hugo Moreau³
Keywords:
Pediatric UTI, Antimicrobial Resistance, Empiric Treatment, ESBL, FranceAbstract
Background:
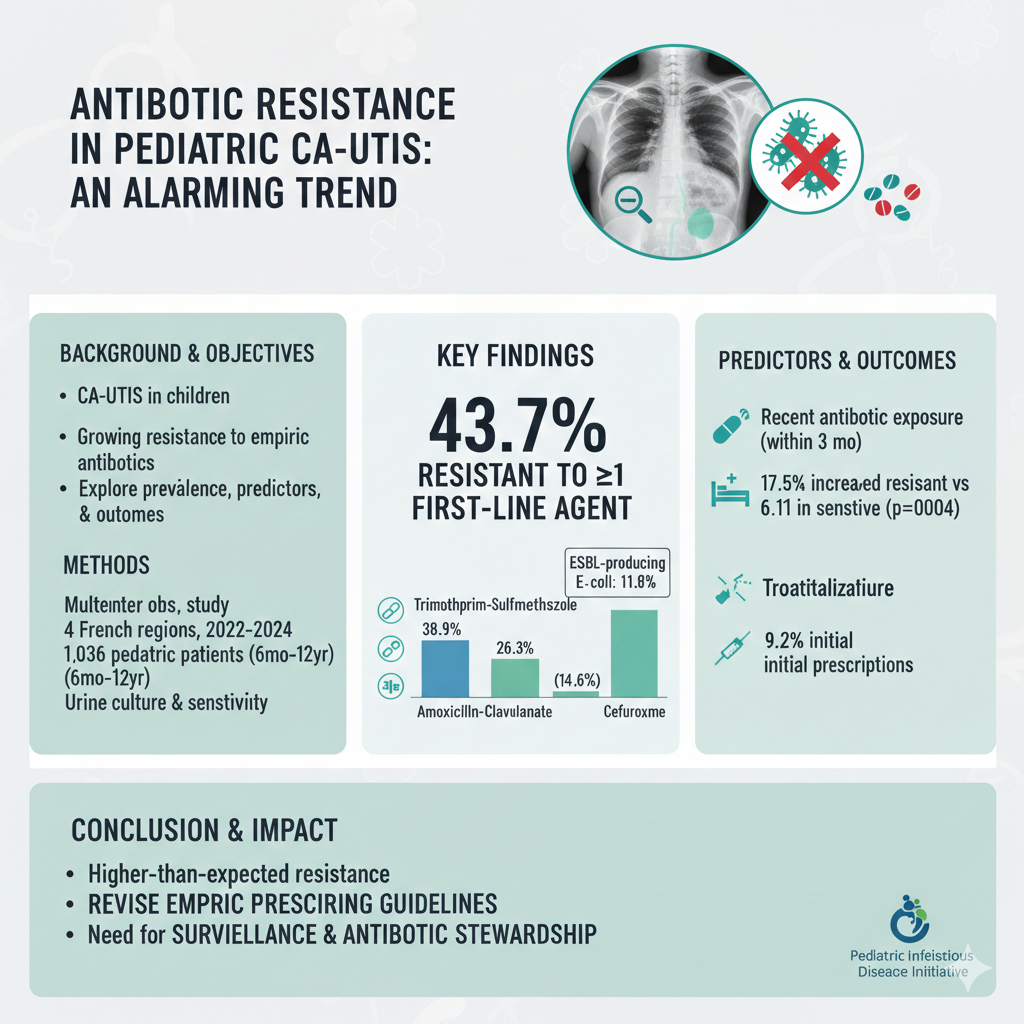
Community-acquired urinary tract infections (CA-UTIs) in children are becoming increasingly resistant to empirical antibiotics. The trend is subtle but alarming, with major implications for outpatient treatment policies and resistance containment.
Methods:
A multicenter observational study was conducted in four regions across France from March 2022 to January 2024. A total of 1,036 pediatric patients (age range: 6 months to 12 years) with CA-UTIs were enrolled. Midstream urine samples were collected prior to treatment, and culture sensitivity testing was performed. Primary outcome was resistance to first-line empiric antibiotics (amoxicillin-clavulanate, trimethoprim-sulfamethoxazole, and cefuroxime).
Results:
Overall, 43.7% of isolates were resistant to at least one first-line agent. Resistance was highest to trimethoprim-sulfamethoxazole (38.9%), followed by amoxicillin-clavulanate (26.3%), and cefuroxime (14.6%). Extended-spectrum beta-lactamase (ESBL)-producing E. coli was detected in 11.8% of cases. Children with recent antibiotic exposure (within 3 months) had a 2.3-fold increased likelihood of resistant infection (p < 0.001). Hospitalization was required in 17.5% of resistant cases versus 6.1% of sensitive cases (p = 0.004). Treatment failure occurred in 9.2% of initial prescriptions, with subsequent switch to broader-spectrum agents.
Conclusion:
The rate of antibiotic resistance in pediatric CA-UTIs is significantly higher than previously estimated, particularly for commonly prescribed oral agents. These findings call for immediate revision of empiric prescribing guidelines in pediatric primary care. Surveillance systems and antibiotic stewardship in outpatient settings are urgently needed to curb rising resistance trends.
Downloads